What Does “Ambiguous Genitalia” Mean?
Sex organs develop with three basic steps. If something goes wrong with this process, a sexual development disorder (DSD) can happen. DSDs are caused by hormones. Genitals can develop in ways that aren’t normal looking. They can be unclear or “ambiguous.” A baby can have features from both genders. The medical term “intersex” is also used to describe ambiguous genitals.
The sex of a baby can be tested to help parents raise a child. Surgery can be used to help clarify a baby’s gender.
Please note: DSD’s are not the same as transsexualism. A transsexual is a person who doesn’t see themselves as their defined gender. DSD’s are different. They are caused by hormones that change the way a fetus develops.
How Do Genitalia Normally Form?
Sex organs develop with three basic steps:
- The genetic sex is set when the sperm fertilizes the egg. An XX pair of chromosomes means that the baby is female. An XY pair means that the baby is male.
- Next, gonads (sex glands) form into either testis for a boy or ovaries for a girl.
- Then, the inner reproductive system, and outer genitals develop. Hormones from either the testis or ovaries shape the outer genitals.
At conception, the mother shares an X chromosome and the father an X or Y chromosome. The pair creates either a female embryo (XX), or a male embryo (XY). At this point, the male and female embryos look the same.
Embryos start with two gonads. They can become either testes or ovaries. Each embryo also starts with both male and female inner genital structures. They become male OR female reproductive structures.
For girls, very little change is needed for the vagina to look normal. The vagina forms right away, before the ovaries have fully formed. For boys, a series of steps must take place. This starts with the growth of testes. The cells of the testes must begin to make testosterone, the male hormone. Then a more powerful hormone (dihydrotestosterone or DHT) causes genital tissues to change. It forms the slit-like groove of the urethra. Then the penis, which was first the size of a clitoris, becomes larger. The tissue on either side forms into the scrotum. Later, the testes move down into the scrotum. At the same time, structures known as mullerian ducts form inner organs. They either become fallopian tubes and a uterus (in a girl), or disappear (in a boy).
All of these steps take place during the first three months of pregnancy. After that, the outer sex organs look like either a penis or vagina.
DSDs can be passed down from a parent, or have no clear cause.
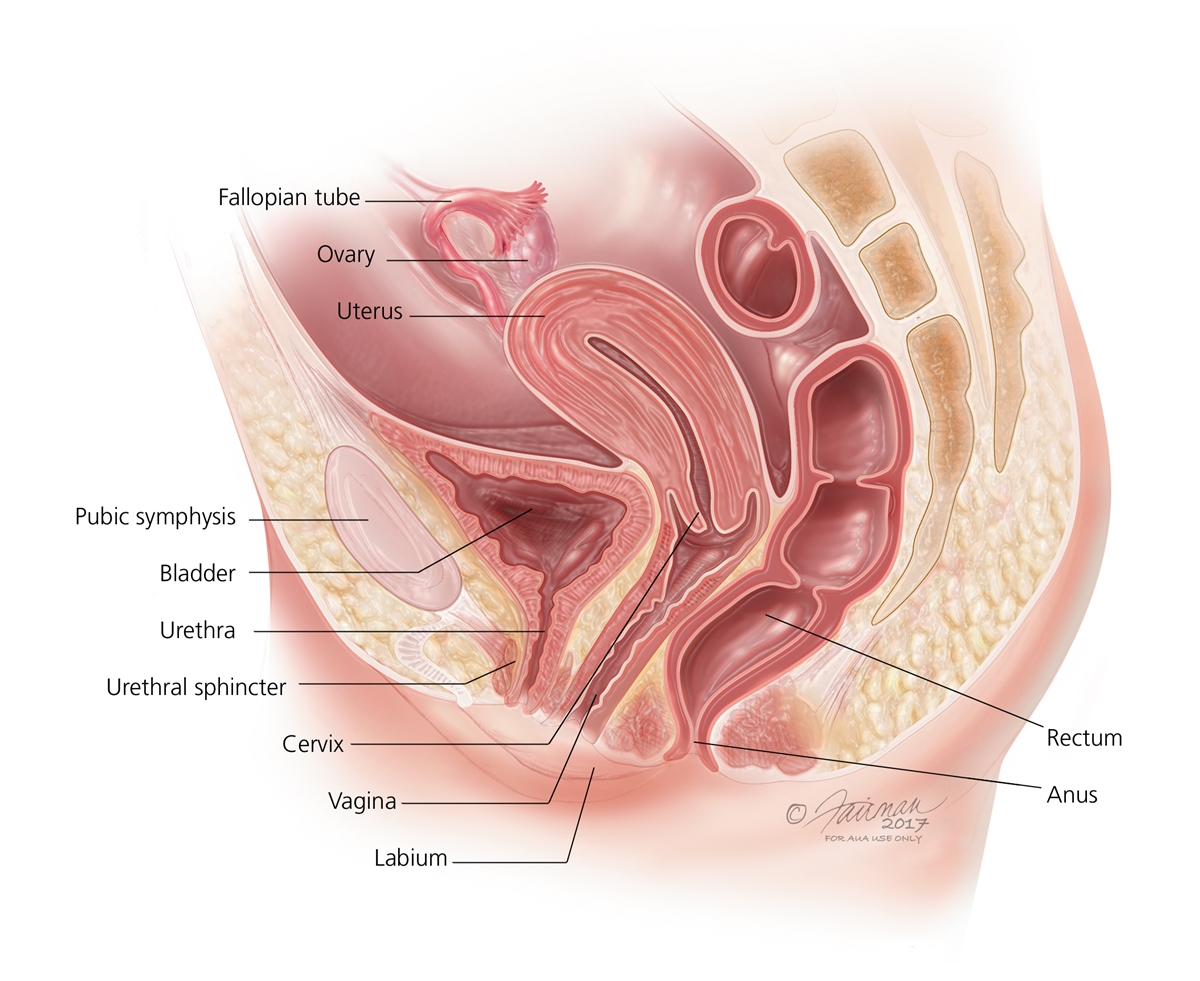
Diagram of the Female Reproductive System
Enlarge
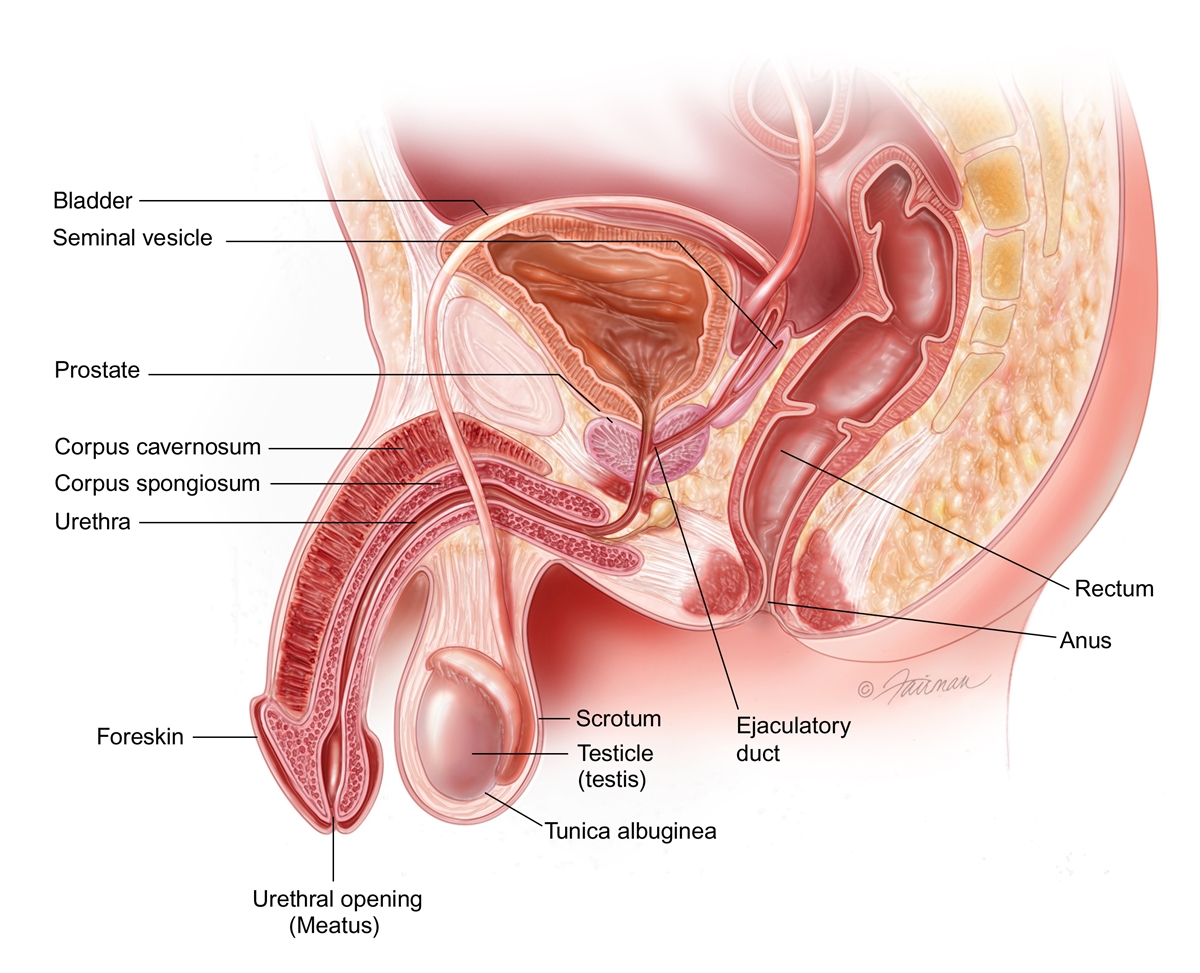
Diagram of the Male Reproductive System
Enlarge
DSDs can cause a range of problems. Some of the signs include:
- Sex organs that don’t look male or female
- Menstruation can begin at an odd age
- Hormonal or electrolyte imbalances
- Hypospadias can form. This is where the penis opening is not at the tip, and the testes have not dropped
46XX DSD
With 46XX, the inner organs are female (the ovaries are normal) but the vagina looks masculinized. This is caused by too many male hormones. Some causes are:
- Congenital adrenal hyperplasia: A common DSD. Too many male hormones cause a girl’s external sex organs to become too large. The clitoris can grow to look like a penis. Another issue is the vaginal opening may not be visible. Hormone and enzyme levels are off-balance. The body’s level of cortisol may be far too low.
- Placental aromatase deficiency: This is from a rare enzyme problem in the placenta. It causes the fetus to get too much testosterone.
- Hormonal medications: Sometimes pregnant mothers are given hormones during pregnancy. They can masculinize the fetus.
- Maternal hormonal imbalance: A pregnant mother can, herself, have a hormone imbalance. This may give the fetus too much testosterone.
46XY DSD
With 46XY, the gonads become testes, but the appearance of the penis is unclear. The cause may be from:
- Testosterone biosynthesis defect: One of the testis’ five enzymes that usually build testosterone, is missing or low.
- 5a-reductase deficiency: There is a low level of the 5a-reductase enzyme. This enzyme is found in male gonads. Without it, testosterone can’t create enough DHT to make male sex organs.
- Partial androgen insensitivity syndrome: In this problem, the cells of the body are only a little responsive to testosterone.
- Complete androgen insensitivity syndrome: In this problem, the body’s cells are not responsive to testosterone. The outer genitalia look female.
Disorders of Gonadal Differentiation
In these cases the gonads may not fully develop into testes. There are three types:
- Mixed gonadal dysgenesis: In this case, one gonad stays premature. The other has formed a testis.
- Partial gonadal dysgenesis: The gonads formed some testicular tissue, but not fully. The testes can’t work properly.
- Gonadal dysgenesis: In this case, both gonads stay premature. They do not become testes.
Ovotesticular DSD
In this rare case, the gonads have both ovarian and testicular tissue. Sometimes there is an ovary on one side and a testis on the other.
Many times it’s clear to see when there’s a gender problem. In other cases, it’s not so simple. Most children are diagnosed at birth. Sometimes a DSD is not found until the teen years.
To make a proper diagnosis, and define a child’s gender, there are tests.
These include:
- A physical exam of outer sex organs
- Blood tests to show your child’s chromosomes and hormone levels
- Ultrasound or MRI tests to see the internal organs
- A genitogram to view inner sex organs. This includes X-rays and catheterization of the openings between the genitals and anus. This will show the urethra and the size of a vagina, if present. This test is helpful for planning surgery.
- Dye may be used
- A biopsy, to test the gonad tissue under a microscope
- In rare cases, gene probe studies may help
- For example, studies of the chromosomes with karyotyping will help define a 44XY DSD
Often, very high or low hormone levels are found in the blood. This tells your doctor the cause of the DSD. Once recognized, hormone levels can often be corrected.
A clear diagnosis will help define sexual function and fertility. Also, it will help parents know what to expect at puberty. All of this helps when defining the baby’s gender and finding treatment.
The first step is to understand the child’s gender. The next step is to consider treatment and support for the child’s emotional well-being.
Treatment depends on what caused the problem. Treatment often involves reconstructive surgery. This would remove or create appropriate sex organs. Surgeons with experience can offer very normal looking results. Hormone replacement therapy (HRT) is also often part of the treatment plan.
For girls with mild congenital adrenal hyperplasia, surgery may not be needed. Hormone therapy may be all that she needs. When the imbalance is managed, she can live a normal life. If the vagina is blocked, surgery would help. This is often done within the first 12-18 months of life.
With vaginal surgery, care is taken to protect clitoral sensitivity. The goal is to prevent injury to the sensory nerves and blood supply. Often, a new opening with vaginal surgery is thin. More surgery may be needed as the child grows. Or, exercises to “stretch” the opening may be done before sexual activity begins.
Surgery for boys with severe hypospadias is often successful. It forms a longer, free penis that can look normal. Any separation of the scrotal sacs would be repaired at the same time. Surgery is done in one or two stages between 6 and 18 months of age. Once healed, the penis grows in pace with normal physical growth. Surgery doesn’t harm a boy’s ability to feel sensation or have an erection.
All credit goes to https://www.urologyhealth.org/urology-a-z/a_/ambiguous-(uncertain)-genitalia